
Physiopathology
The cyst of the septum pellucidum(CSP) occurs in the centerof the corpus callosum at the 3th month of gestation.
At approximately the 6th month of gestation, the cavum begins to close in a caudal-to-rostral direction and several months after the birth normally CSP disappears.
However, abnormalities in the closing of the CSP cavity are seen in 0,3-1,75% of cases on post-natal CT scans. These close-down imperfections of CSP are usually thought to be a variation of normal anatomy and most cases are asymptomatic.
Lissand Mervis described three variations of the septum pellucidum:
Nonneoplastic cysts of the septum pellucidum are of two general forms.
The first, the asymptomatic cavum septum pellucidum, is a common incidental finding during imaging of the central nervous system and maybe associated with a cavum vergae or cavum velum interpositum. Incidence: 20.3% with a slightly higher in males, in professional boxer sand patients with schizophrenia.
The second form of non neoplastic cystis the true septum pellucidum cyst. This represents an abnormal symptomatic expansion of a cavum septum pellucidum (expanding cyst of septum pellucidum). Because there are no radiographic criteria for identifying a true septum pellucidum cyst, its distinction is based on the development of neurological symptoms in association with the expansion of an existing cavum.
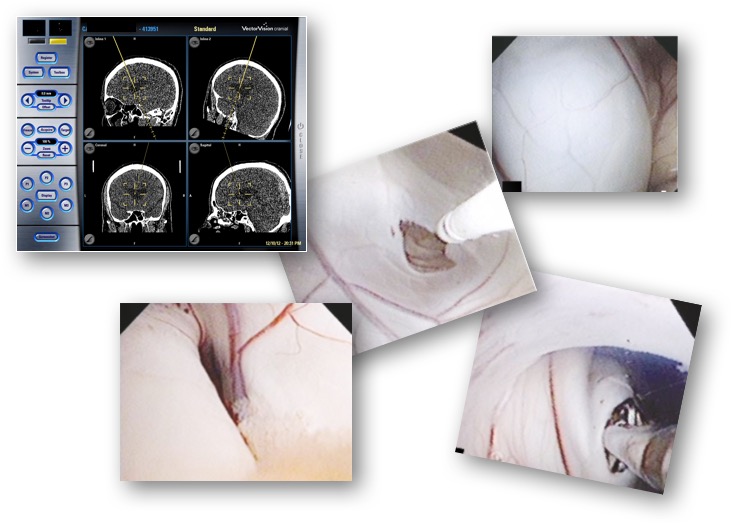
Endoscopic fenestration of symptomatic septum pellucidum cysts produces immediate relief of the mass effect of the cyst and resolution of associated symptoms.
Cannulation of the lateral ventricle before cyst fenestration prevents inadvertent injury to the fornices, thalamus, internalcapsule, caudate nucleus, and septal and thalamostriate veins.
